The story of demographic doom has become familiar: Declining birth rates will cause populations to shrink, while longer lifespans will increase the costs of pensions and eldercare. Relatively fewer workers will have to pay for it all.
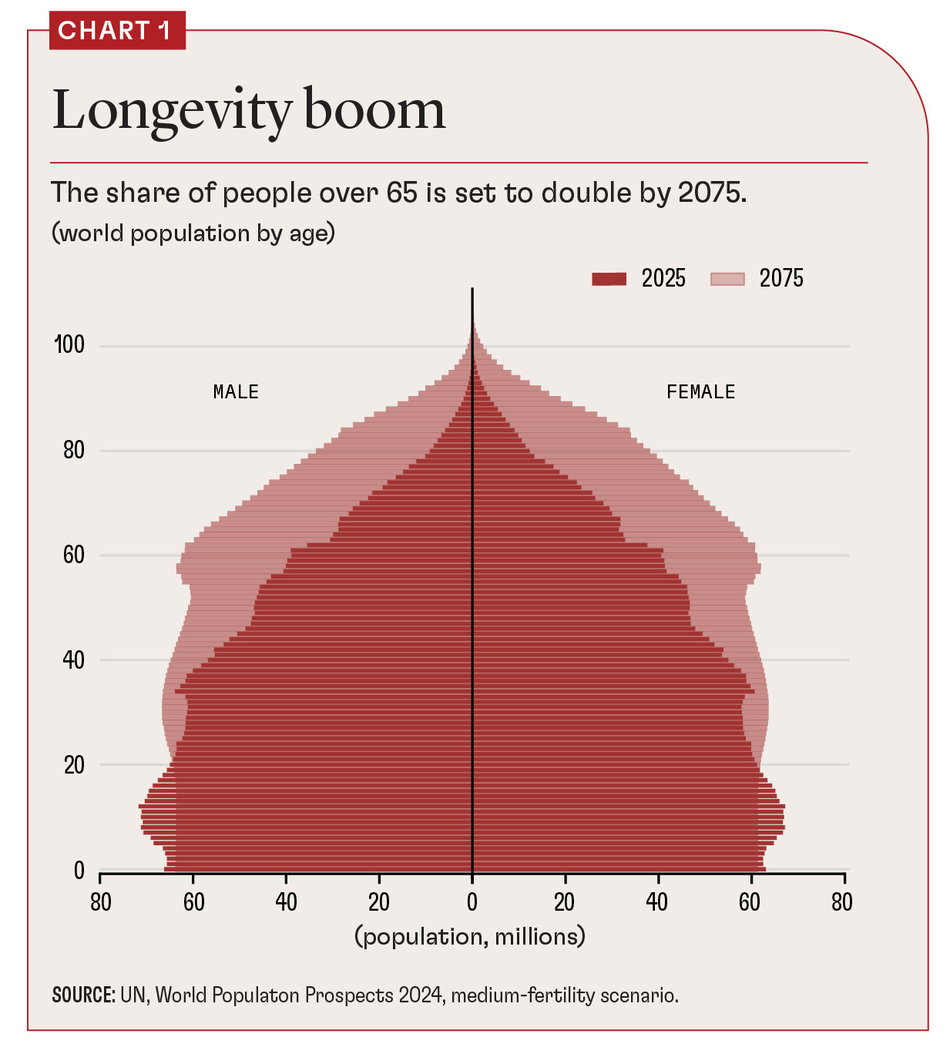
This story is partly true: One in ten people worldwide are now over 65, and that proportion is projected to double over the next 50 years (see Chart 1). Population decline has already begun in places such as Japan and China. Those countries are also experiencing a sharp increase in median age, as is Europe.
But the pessimism around an aging population is too one-sided. In fact, the combination of older people becoming more numerous and more likely to work makes them essential to economic dynamism.
In Europe, 90 percent of the increase in workers in the past decade—17 million more people in employment—came from a jump in workers over 50, according to the Organisation for Economic Co-operation and Development. In Japan, the proportion is even higher. In both places, older workers are already the main driver of GDP growth.
This is just one component of the “longevity dividend” societies can reap if we rethink our approach to aging (Scott 2024). It starts with reframing the policy debate in two fundamental ways.
The first is to stop seeing an aging society only as a problem. This is a strikingly negative way of framing one of the greatest achievements of the 20th century: Most of humanity is living longer, healthier lives. That’s an opportunity.
The second is to drop the unworkable focus on changing individual behavior in order to preserve current systems. Instead, focus on helping each person adapt to greater life expectancy—give them the support needed to live their best longer life.
This perspective points us to a new approach to aging based on redesigning health systems and investing more in our later-life human capital to seize the opportunities of an older, more experienced population.
Adapting to longevity
In the 20th century, more people living from 40 to 60 meant more years when people tended to be employed and in reasonably good health. In this century, life expectancy gains mean more people living from 60 to 90. If people’s behavior doesn’t change and systems are still based on the life expectancy of the previous century, pension and health costs will rise and be a drag on economies, especially those of richer countries.
For individuals, longer life causes a profound change in outlook. When there is only a small chance of living long enough to become old, investing to benefit your future octogenarian self doesn’t make sense. But with global life expectancy now exceeding 70, and even 80 in an increasing number of countries, it does.
This logic has radical implications for our health, education, work, and financial systems—areas where traditional approaches are no longer working.
Raising the state retirement age generates widespread resistance. Policies aimed at raising birth rates are expensive and have relatively modest effects because they go against individual preferences. Immigration holds political challenges.
What’s more, the latter two sets of policies target changing the relative size of different age groups but do not address the deeper challenge of how we adjust to longer lives. If longevity is what makes our pensions and health systems unsustainable, higher birth rates or immigration merely delay the financial day of reckoning.
Investing in the human and social capital of our later years is the only sustainable solution to the challenges of an aging society.
Expansion of morbidity
Gains in life expectancy over the previous century drove an epidemiological transition, with the health burden shifting from infectious to chronic noncommunicable diseases (Omran 1971). The latter now account for 60 percent of the disease burden globally, and 81 percent in the European Union.
Because of this shift in the disease burden, healthy life expectancy has not grown as fast as overall life expectancy, causing an expansion of morbidity. The current health system is at risk of keeping us alive but not healthier for longer, at an ever-increasing cost to individuals, families, and society.
In short, in the 20th century, we added years to life. In the 21st, we must add life to these extra years.
This requires a shift toward chronic disease prevention and health maintenance, not just treating people when they become ill. Three factors make the switch to prevention more feasible and desirable.
First, increased longevity means that most people can expect to experience chronic disease.
Second, the growing availability of structural risk and genetic data makes targeted interventions possible. Given the significant role of socioeconomic factors in driving health, this points to a clear link between reducing poverty and improving a country’s health as well.
Third, advances in biology hold the prospect of more effective forms of prevention. The dramatic impact of GLP-1 drugs such as Ozempic and Wegovy shows how a single class of therapeutics can help postpone the incidence of multiple diseases. Likewise, developments in the biology of aging hold the potential for future drugs that tackle aging-related diseases directly.
Increased investment in life sciences and biopharmaceuticals should lead to the development of these therapies, as well as to modes of prevention that work better and are more cost-effective. Promising areas include improved vaccines for older people that exploit potential gains in geroscience, cancer therapies, synthetic biology, and genomics.









